
Table of Contents
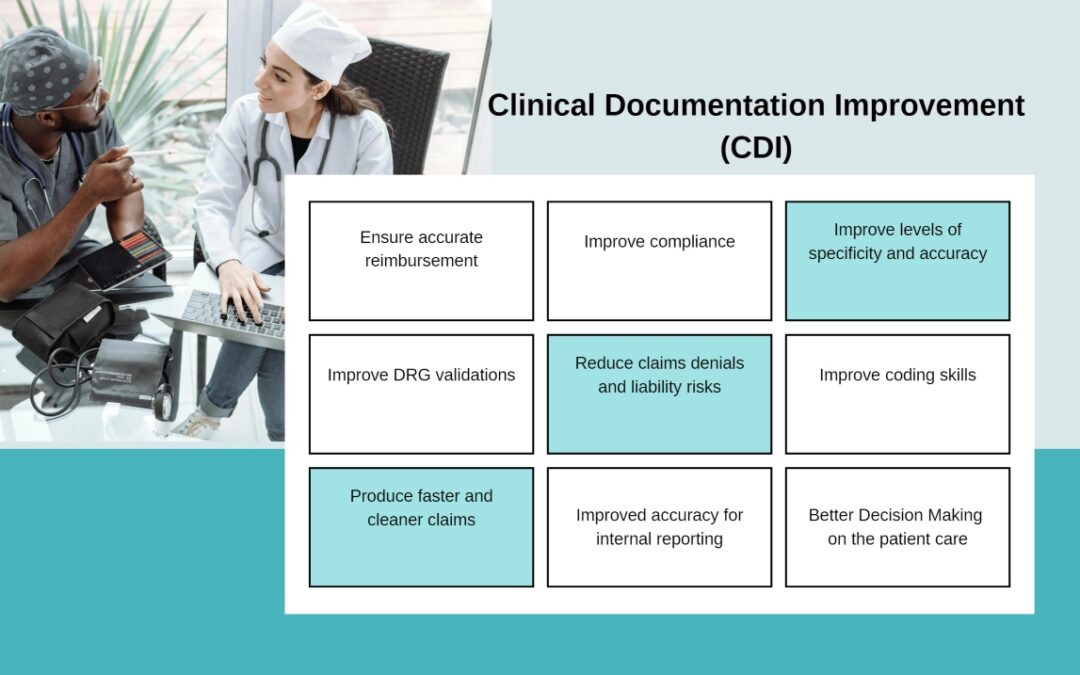
What is Clinical Documentation Improvement (CDI)
Clinical Documentation Improvement (CDI) is an important practice in the healthcare business that aims to improve the quality and completeness of patient data. The CDI practice involves checking the accuracy and completeness of the documentation found in medical records. CDI includes the diagnostic results, illness process, and any potential gaps in the documentation.
Physicians, dentists, chiropractors, and other healthcare professionals may write entries in the medical record. In certain situations, who can document in the medical record may be limited by regulations, accreditation criteria, corporate policies, and other guidelines. A CDI specialist should be experienced in both clinical and medical coding procedures. He should ensure to keep records up to date through real-time documentation of care and changes in patient conditions.
What a CDI Program Is For:
A clinical documentation improvement program is a methodical, structured procedure designed to provide accurate disease process, diagnostic results, and complete documentation of medical records. Managing administrative duties associated with patient care and claim submission has become easier for hospitals and providers because to the use of EHR systems. Healthcare companies may maintain their forefronts in Clinical Documentation Improvement (CDI) by adopting the emerging trends (like artificial intelligence) and using technology to improve patient care and operational effectiveness. Clinical Documentation Improvement training frequently includes topics such as efficient contact with healthcare professionals and the use of technology to streamline documentation procedures.
The Effects of a CDI Program in an Inpatient Environment
CDI can make significant contribution to inpatient facilities’ coding and billing procedures, and right compensation. Nevertheless, a clinical documentation improvement (CDI) program’s make financial impact on an inpatient environment extends beyond the initial claim payment. Erroneous claims made due to poor documentation may result in an adverse audit, requiring facilities to pay a penalty or return money they unintentionally obtained from payers. CDI coding enables companies to comply with coding standards and regulations, lowering the risk of auditing and penalties. Thus, for claims processing at healthcare facilities, CDI is evident in two domains.
- The first is the increase in initial compensation accuracy,
- The avoidance of expensive consequences as a result of authority evaluations.
How Can Clinical Documentation Improvement (CDI) Enhance Patient Care?
The cost implications of an inpatient CDI treatment are but one aspect of it. Another important factor is the improvement of each patient’s record, which contributes to the overall well-being of the patient population. Because it affects continuity and quality of service, inadequate documentation can have an impact on how a healthcare facility treats its patients. Examining the paper with other healthcare professionals who are involved in the patient’s care, such as physicians and medical teams, facilitates better communication between all parties involved in providing patients with prompt services, potentially reducing the length of time they spend in the hospital.
Payers have recognized these benefits and created programs to support them. Moreover, CDI program could help in to reduce avoidable readmissions by improving communication and care harmony among patients and their caregivers upon discharge. A value-based purchasing initiative that reduces payments to hospitals that have too many readmissions is the HRRP (Hospital Readmissions Reduction Program). CMS assesses various healthcare actions that have an impact on patients’ health in collaboration with HRRP. Moreover, CDI software and technology play an important role in streamlining operations and assisting healthcare providers with their overall goals.
The effects of a program for clinical documentation improvement (CDI) in an outpatient setting
Even though an outpatient CDI program may not have the same financial impact as an inpatient program, provider offices nonetheless need to implement it. They rely on these locations’ income cycle, just like hospitals, to cover costs and remunerations. It can be problematic to receive payment for rendered services on schedule when claims are denied or altered as a result of submitting the wrong code. In an outpatient context, the primary goal of a physician’s CDI plan is to halt these alterations and repudiations while making sure that mentation is complete for therapeutic purposes.
Also, the integration with EHR systems ensures that CDI activities are in sync with the whole healthcare workflow, allowing for real-time documentation and interaction among healthcare practitioners. CDI specialists play an important role in quality improvement programs. They give data and insights from documentation analysis, which can be utilized to discover areas of enhancement of patient care and operational efficiency.
Improved Quality of Patient Records:
The two primary objectives that clinicians face when managing a practice are diagnosing patient problems and providing appropriate therapy. A clinical record can be thought of as a language in its entirety. Since their speech has an impact on how others interpret what they write or type, they must talk clearly and appropriately. Care pathway navigators, patients, healthcare providers, and network management are the ones who adhere to the language. Patients find it simpler to receive the care they require from various sources during their medical journey when CDI is enhanced. Good communication with patients reduces the likelihood that they will be misunderstood or misinterpreted, which benefits the practice.
Appropriate Payment With Proper CDI
All organizations, (regardless of size), require a healthy level of revenue, which can be achieved with the proper CDI. Similarly, proper clinical documentation leads to accurate coding and payment from service payers. A solid basis in clinical knowledge, such as medical terminology, anatomy, and physiology, is essential for correctly understanding and reporting medical data.
CDI’s Prospects and Future Directions for Improving Patient Care
With the introduction of cutting-edge technology like artificial intelligence (AI), the future of CDI is full with potential opportunities. These developments could further improve documentation procedures, which would benefit patients and the healthcare system as a whole. In order to find trends and recommend changes in documentation, AI algorithms can evaluate enormous volumes of clinical data. This results in patient records that are more thorough and accurate. Proactive healthcare management can be supported by improving care quality and identifying areas for documentation improvement by utilizing data analytics to forecast patient outcomes. As telehealth becomes more common, CDI programs must evolve to ensure proper recording of virtual appointments and remote patient monitoring data. The use of electronic health record (EHR) systems and other digital tools to ensure accurate and efficient record-keeping.
Wrap Up
Clinical Documentation Improvement (CDI) initiatives are essential for maintaining accurate medical records. This is required for both long-term and short-term treatment facilities, such as clinics or other outpatient healthcare settings. Clinical Documentation Improvement programs help to increase the precision of coding and invoicing, ensuring that everything is done correctly and no wrong payments are received.
Read More: Understand the Frequently Used Physical Therapy Modifiers?